
"The Treatment Exists But Not for Patients Like Me”: The Evidence Gap Behind Cancer Care Inequality
- Apr 27
- 5 min read

In oncology, the concept of evidence-based care carries a certain weight. It signals rigor, validation, and a level of certainty that both clinicians and patients rely on when making decisions that are often time-sensitive and high stakes.
However, what is less frequently examined is the context in which that evidence is generated, and how closely it aligns with the realities of patients receiving care outside of those controlled environments.
For many patients, particularly those treated in community settings rather than large academic centers, there is an emerging disconnect that is not always immediately visible, but becomes more apparent over the course of treatment. It is not a question of whether therapies are effective in principle, but rather how consistently that effectiveness translates across different clinical, social, and economic contexts.
Most Oncology Evidence Is Built In Controlled Settings That Do Not Reflect Real-World Care
Much of modern oncology has been shaped by randomized controlled clinical trials designed to isolate therapeutic effect under highly specific conditions, where patient populations are carefully selected, comorbidities are often minimized, and access to diagnostics and specialist care is assumed rather than variable.
These conditions are essential for establishing efficacy, but they also create a version of the patient journey that is inherently simplified compared to what is observed in broader care delivery environments.
In contrast, a substantial proportion of oncology care is delivered in settings where patients present later in the disease pathway, where multiple chronic conditions are the norm rather than the exception, and where access to diagnostic tools, specialist input, and consistent follow-up can vary significantly depending on geography, infrastructure, and socioeconomic factors.
It is within this contrast that the misalignment begins to take shape, not as a flaw in the science itself, but as a limitation in how far that science extends once it leaves the controlled setting in which it was generated.
Small Differences Between Trials And Practice Can Compound Into Meaningful Outcome Gaps
When viewed in isolation, the differences between clinical trial environments and real-world care settings can appear incremental. However, when considered together, they begin to form a pattern that has meaningful implications for how therapies perform outside of the contexts in which they were validated.
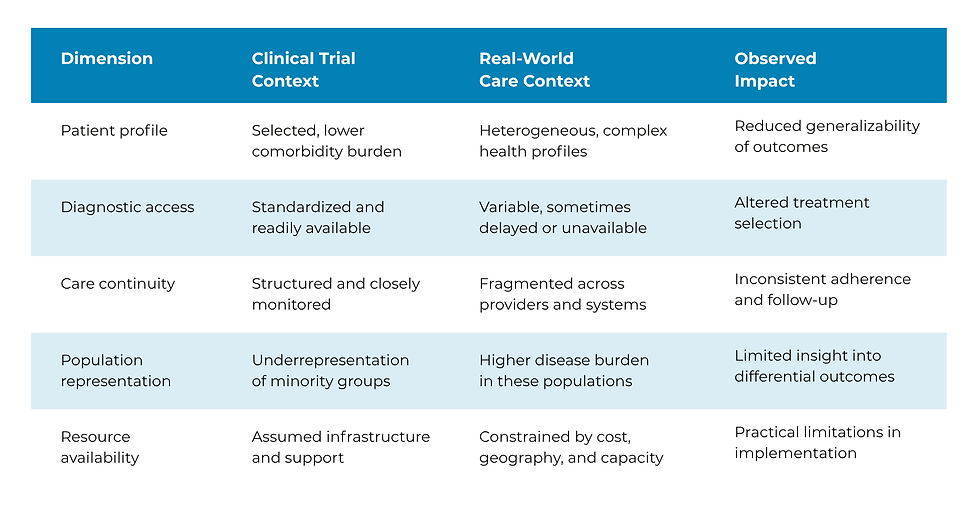
Taken together, these differences do not simply introduce variability, they reshape the conditions under which care is delivered, often in ways that are not fully accounted for in trial design or interpretation. As a result, the application of evidence becomes less about direct translation and more about adaptation, frequently without the supporting data needed to guide that process with confidence.
Modern Therapies Depend On Infrastructure And Consistency That Many Patients Do Not Have Access To
The divergence between evidence and practice tends to be more pronounced in areas where therapies rely on precision, infrastructure, or consistency of delivery, all of which are sensitive to variations in care environments.

There is a growing body of evidence suggesting that these gaps are not incidental, but structural. Studies have shown that minority populations continue to be underrepresented in oncology clinical trials relative to their disease burden (Loree et al., JAMA Oncology, 2019), and that patients treated outside academic centers may experience different outcomes compared to those treated within them (Unger et al., Journal of Clinical Oncology, 2014).
Additionally, the exclusion of patients with comorbidities, a common feature of trial design, has been shown to limit the applicability of findings to broader patient populations (Kim et al., Cancer, 2015), reinforcing the idea that current evidence frameworks, while methodologically sound, do not fully capture real-world complexity.
At the same time, smaller-scale, practice-led pilot programs are beginning to surface a different dimension of the problem, one that sits outside traditional clinical trial design but directly impacts outcomes.
In a community oncology setting, the “No One Left Alone (NOLA)” pilot program demonstrated that a significant proportion of barriers to cancer care were not clinical, but financial and logistical. By embedding dedicated support staff within the practice to help patients access drug assistance programs and navigate cost-related barriers, the initiative generated over $1.7 million in financial support and reached nearly half of the clinic’s patient population.
These types of pilot interventions are not testing new therapies, they are testing whether addressing real-world constraints around access, affordability, and care coordination can materially improve outcomes without changing the treatment itself.
Patients Experience This Gap As Uncertainty, Not As A Clinical Trial Limitation
Although these issues are often discussed in methodological or statistical terms, their impact is ultimately experienced at the patient level, where decisions are made within the constraints of what is feasible rather than what is ideal.
This can manifest as adjustments to treatment plans based on access to diagnostics, interruptions in therapy due to financial or logistical barriers, or outcomes that diverge from expectations established in clinical trial settings.
For patients, this does not necessarily present as a loss of confidence in the system, but rather as an awareness that the evidence guiding their care may not fully account for the conditions in which that care is delivered.
Community Practices Treat The Most Representative Patients But Remain Excluded From Evidence Generation
A significant proportion of oncology care, particularly among underserved populations, is delivered in community-based practices that operate with a different set of constraints and patient demographics compared to large research institutions.
These settings are characterized by greater variability in patient presentation, resource availability, and care pathways, yet they remain underrepresented in the clinical trial ecosystem and in the data that informs future standards of care. This creates a structural imbalance in which the environments that most closely reflect real-world patient experiences contribute the least to the evidence base that defines how care should be delivered.
What these pilot programs make increasingly clear is that the same community settings capable of identifying and addressing real-world barriers are also those least integrated into evidence generation. In effect, the environments that most accurately reflect patient reality are still peripheral to how oncology data is built.
Closing Evidence Gaps Requires Building Data In Real-World Settings And This Is Where Rubix LS Operates
The industry has made significant progress in developing therapies that demonstrate clear efficacy under controlled conditions, and that foundation remains critical to advancing oncology care.
What is becoming increasingly clear, however, is that the next phase of progress will depend on expanding how evidence itself is generated, so that it captures not only what is scientifically possible, but also what is consistently achievable across the full spectrum of patients, care settings, and real-world constraints.
At Rubix LS, this is where we see our role, not as an observer of this shift, but as part of the infrastructure needed to support it. We work at the intersection of clinical research, care delivery, and real-world context, helping to bring community-based practices, underserved patient populations, and operational realities into closer alignment with how evidence is generated and applied. By bridging these environments, the goal is not only to expand access to trials, but to ensure that the data emerging from them more accurately reflects the patients and systems they are ultimately intended to serve.
If this is an area your team is actively exploring, whether from a clinical, operational, or investment perspective, we welcome the opportunity to continue the conversation.
Connect with the Rubix LS team to explore how evidence generation can better reflect real-world care.


